Introduction
Congenital renal fusion anomalies represent an uncommon spectrum of developmental abnormalities arising from aberrant ascent and rotation of the metanephric blastema during embryogenesis [1]. Among these anomalies, pancake kidney (PK) (also referred to as disc, doughnut, shield, or cake kidney) is exceptionally rare and constitutes the most extreme variant of crossed-fused renal ectopia. It is characterized by complete medial fusion of both kidneys into a single flat discoid mass. It is typically located deep within the pelvic cavity and has short ureters, anteriorly facing pelvicalyceal systems and highly variable vascular anatomy. The arterial supply to PK commonly originates from distal aortic or iliac branches rather than the usual renal arteries complicating both diagnostic evaluation and surgical planning in these cases [2].
Most patients with PK remain asymptomatic and it is often detected incidentally on imaging or during surgery for unrelated conditions. However abnormal urinary drainage, pelviureteric malorientation, and stasis usually predispose these patients to complications. These complications include recurrent urinary tract infections, hydronephrosis and nephrolithiasis which is the most frequently reported clinical manifestation. The simultaneous occurrence of renal calculi with vesical calculus in pancake kidney remains extremely rare with limited documentation in the existing literature [3].
The management of urolithiasis in pancake kidneys is technically challenging because of the altered anatomy, ectopic pelvic location, unpredictable vascular supply and proximity to surrounding pelvic organs. Conventional percutaneous nephrolithotomy (PCNL) may have limited role in PK cases due to restricted percutaneous access windows as well as increased risk of adjacent organ injury. Endoscopic approaches can be compromised by presence of anomalous calyceal orientation and ureteric kinking. Therefore, traditional open pyelolithotomy carries higher morbidity, extended recovery time and inferior cosmetic outcomes in these cases [4].
The advent of robot-assisted laparoscopic surgery has revolutionized the surgical management of complex renal anatomy. It offers three-dimensional magnified visualization of renal anatomy, articulated instrumentation and comparatively superior dexterity. These advantages allow superior dissection ability around aberrant vessels, precise identification of the collecting system and accurate stone extraction. Emerging evidence supports the safety and efficacy of robotic-assisted pyelolithotomy particularly in cases with anomalous or ectopic kidneys (such as in cases of PK) and complex stone burden [5].
In this report, we describe a rare case of a pelvic pancake kidney with concurrent renal and urinary bladder calculi successfully managed in a single-session robotic-assisted laparoscopic pyelolithotomy combined with cystolithotomy, highlighting both the feasibility and advantages of this minimally invasive approach in managing complex stone disease associated with congenital renal fusion anomalies.
Case presentation
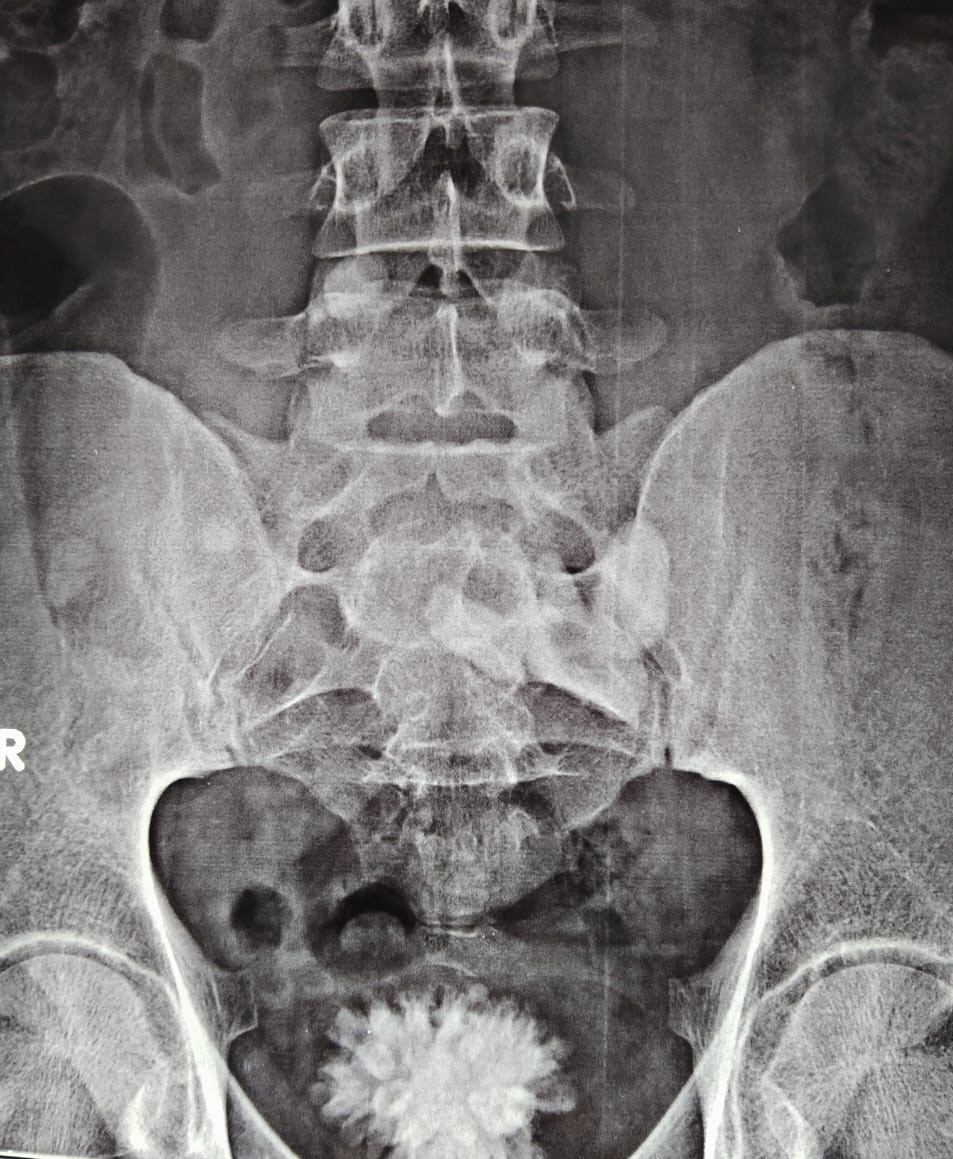
A 27-year-old male presented with suprapubic pain, dysuria, and intermittent haematuria for 7 days. X-ray KUB revealed a bladder calculus, while ultrasound suggested a pelvic fused kidney with renal stones (Figure 1).
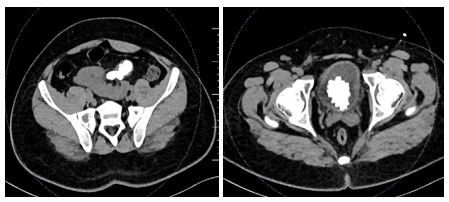
Contrast-enhanced CT KUB demonstrated a single, flat, discoid renal mass located in the pelvic cavity, consistent with a pancake kidney, showing complete fusion of both renal units across the midline with absent renal ascent and malrotation. The collecting systems were anteriorly oriented and the ureters were observed to be short. Within the fused renal moiety, two non-obstructing calculi were identified, measuring approximately 10.8 × 11.7 × 16.3 mm and 7 × 9 × 9.5 mm. There was no associated calyceal dilatation or hydronephrosis. Additionally, a large hyperdense vesical calculus was noted within the urinary bladder (Figure 2).
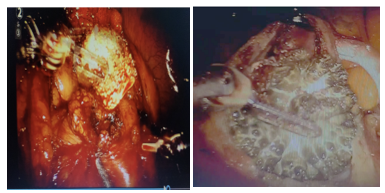
Intraoperatively we first performed cystoscopy for RGP and stenting but owing to the presence of severe mucosal edema we could not find the bilateral ureteric orifice. Therefore, the decision of robotic-assisted laparoscopic pyelolithotomy and cystolithotomy was made. The kidney was intraoperatively located with intraoperative ultrasound, retroperitoneal dissection was performed, pyelolithotomy was performed, the stones were removed with the needle holder. The bladder was dissected, a horizontal incision was made over the bladder, and cystolithotomy was performed followed by bladder stone removal. Then, retrograde DJ stenting was performed with an extensive search for the bilateral ureteric orifice. Robotic assisted pyeloplasty and bladder reconstruction were performed after bladder washing. We placed 22 fr abdominal drains in the left lumbar region with a 16 fr Foley’s catheter. (Figure 3).
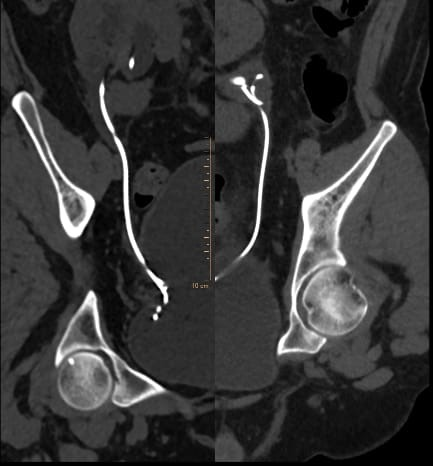
Postoperatively, the patient was vitally stable without any complications. The drain was removed on the third day, and catheter removal was performed after 7 days. Low-dose KUB CT was performed after 6 weeks for any remaining stone fragments, suggesting complete clearance , and bilateral DJ stent removal was performed after 6 weeks
Discussion
Pancake kidney is a rare congenital renal fusion anomaly which is characterized by complete fusion of both kidneys into a single discoid pelvic mass with associated malrotation and anterior displacement of the collecting systems. These anatomical features predispose patients to urinary stasis, recurrent infection and nephrolithiasis. Despite being mostly asymptomatic and incidentally detected, symptomatic cases pose significant diagnostic and therapeutic challenges due to limited surgical access, complex vasculature and proximity to pelvic viscera [6].
Ghawanmeh et al reported a rare pelvic pancake kidney which was incidentally discovered during imaging [7]. Their patient exhibited impaired urinary drainage and recurrent symptoms but was managed conservatively due to a low stone burden. Similarly Lomoro et al described case of a 14-years old female with PK who was misdiagnosed with a horseshoe kidney (HSK) during an abdominal ultrasound [8]. This case highlights the importance of accurate imaging for anatomical delineation and preoperative planning.
A surgically comparable case was reported by Antonelli et al who described successful robot-assisted bilateral pyelolithotomy in ectopic pelvic kidneys. This case demonstrated the role of robotic surgery in reducing technical difficulties which are usually associated with anomalous renal anatomy [9]. The authors reported excellent post-operative outcomes in terms of complete stone clearance and minimal morbidity. The authors concluded that robotic surgery is viable and safe approach for complex stone disease in ectopic kidneys. While their case did not involve a pancake kidney specifically however the operative challenges were similar including pelvic access limitations and distorted collecting systems.
Traditional management strategies for large stone burden in fusion anomalies have favoured open pyelolithotomy. However, this approach is associated with increased postoperative pain, significantly longer hospital stays and greater morbidity. Percutaneous nephrolithotomy (PCNL) in these cases is also technically constrained due to limited safe access and increased risk of bowel injury [10].
Robotic-assisted surgery effectively overcomes these limitations by providing enhanced three-dimensional visualization and by familiarising precise dissection around aberrant vessels and accurate incision of the collecting system. Our successful outcome confirms the findings by Antonelli et al and reinforces the effectiveness of robotic surgery as a first-line surgical option for complex stone disease in patients with anomalous kidneys [9].
Our present case adds unique value to existing literature by demonstrating the practical feasibility of single-session combined robotic-assisted pyelolithotomy and cystolithotomy in a patient with pancake kidney which was further complicated by simultaneous renal and bladder calculi.
Conclusion
Robotic-assisted pyelolithotomy (RAPL) represents a safe and highly effective surgical option for managing nephrolithiasis in patients with pancake kidney. It is particularly important because of complex pelvic anatomy and aberrant vascular patterns. These advantages translate into high stone-free rates with reduced perioperative morbidity as compared to percutaneous nephrolithotomy (PCNL). Our case report shows that RAPL can be considered a first-line therapeutic option for complex stone disease associated with anomalous renal fusion including pancake kidney.
Consent and ethics
Written informed consent was obtained from the patient for publication.
References
- Kubihal V, Razik A, Sharma S, Das CJ. Unveiling the confusion in renal fusion anomalies: role of imaging. Abdom Radiol (NY). 2021 Sep;46(9):4254-4265. doi: 10.1007/s00261-021-03072-1.
- Eckes D, Lawrence P. Bilateral iliac artery aneurysms and pancake kidney: a case report. J Vasc Surg. 1997 May;25(5):927-30. doi: 10.1016/s0741-5214(97)70224-6.
- Tiwari AK, Choudhary AK, Khowal H, Chaudhary P, Arora MP. Pancake kidney: A rare developmental anomaly. Can Urol Assoc J. 2014 May;8(5-6):E451-2. doi: 10.5489/cuaj.1933..
- Kumar S, Bishnoi K, Panwar VK, Kumar A, Sharma MK. Stone in ectopic pelvic pancake kidney: a surgical challenge overcome by robotic surgery. J Robot Surg. 2018 Mar;12(1):181-183. doi: 10.1007/s11701-017-0704-2.
- Tu HA, Weng SC, Lin YH, Chen CL, Chen YT, Juang HH, Hou CP. Comparative Analysis of Surgical Outcomes Between Robotic-Assisted Pyelolithotomy and Mini-Percutaneous Nephrolithotomy for Renal Stones Larger Than 2 cm in Older Adults: A One-Year Follow-Up Study. Int J Nephrol Renovasc Dis. 2025 Jun 17;18:177-185. doi: 10.2147/IJNRD.S532866.
- da Silva RM, de Morais Júnior MF, Mont'Alverne Filho FE. Pancake kidney with cysts and a single ureter. Radiol Bras. 2016 Mar-Apr;49(2):127-8. doi: 10.1590/0100-3984.2015.0063.
- Ghawanmeh HM, Al-Ghazo M, Halalsheh OM, Al-Ghazo OM, Alshammari AK, Al-Karasneh AI, Al-Okour R. Pancake Kidney Found Inside Abdominal Cavity: Rare Case with Literature Review. Urol Case Rep. 2017 May 5;13:123-125. doi: 10.1016/j.eucr.2016.11.020.
- Lomoro P, Simonetti I, Vinci G, Fichera V, Prevedoni Gorone MS. Pancake kidney, a rare and often misdiagnosed malformation: a case report and radiological differential diagnosis. J Ultrasound. 2019 Jun;22(2):207-213. doi: 10.1007/s40477-018-0331-4. Epub 2018 Oct 25.
- Antonelli A, Peroni A, Furlan M, Palumbo C, Zamboni S, Veccia A, Simeone C. Robot-assisted Partial Nephrectomy and Bilateral Pyelolithotomy in Ectopic Pelvic Kidneys. Urology. 2019 Jul;129:235. doi: 10.1016/j.urology.2019.03.025.
- Bapir R, Sabr WN, Tahir SH, Saida BS, Abdullah BA, Hasan KM, Kareem HO, Nasralla HA, Abdalla BA, Hama NH, Kakamad FH. Pancake kidney in infant: A case report with literature review. Radiol Case Rep. 2025 Nov 15;21(2):575-580. doi: 10.1016/j.radcr.2025.10.054.